آخر المواضيع المضافة

 النبات
الحيوان
الأحياء المجهرية
علم الأمراض
التقانة الإحيائية
التقنية الحيوية المكروبية
التقنية الحياتية النانوية
علم الأجنة
الأحياء الجزيئي
علم وظائف الأعضاء
الغدد
المضادات الحيوية
النبات
الحيوان
الأحياء المجهرية
علم الأمراض
التقانة الإحيائية
التقنية الحيوية المكروبية
التقنية الحياتية النانوية
علم الأجنة
الأحياء الجزيئي
علم وظائف الأعضاء
الغدد
المضادات الحيوية| NOCARDIOSIS |


|
|
Read More
Date: 18-3-2016
Date: 2025-01-01
Date: 10-3-2016
|
The genus Nocardia continues to undergo extensive taxonomic reclassification. New species continue to be recognized, and at least 30 species have been implicated as causes of human infections.
The most common species associated with the vast majority of cases of human infections are listed in Table 1. Each of these is responsible for a broad range of diseases, and each species or complex has unique drug susceptibility pat terns. The pathogenic nocardiae, similar to many nonpathogenic species of Nocardia, are found worldwide in soil and water. Nocardiosis is initiated by inhalation of these bacteria. The usual presentation is as a subacute to chronic pulmonary infection that may disseminate to other organs, usually the brain or skin. Nocardiae are not transmitted from person to person.

Table1.
Morphology and Identification
Nocardia species are aerobic and grow on a variety of media. Microscopically in clinical specimens, nocardiae appear as filamentous organisms with hyphae-like branching. On standard laboratory media, after incubation at 35–37°C for several days, they develop heaped, irregular, waxy colonies. Strains vary in their pigmentation from white to orange to red. These bacteria are gram positive and catalase positive, and they produce urease. Nocardiae form extensive branching substrates and aerial filaments that fragment, breaking into coccobacillary cells. The cell walls contain mycolic acids that are shorter chained than those of Mycobacteria. They are considered to be weakly acid fast, that is, they stain with the routine acid-fast reagent (carbolfuchsin) and retain this dye when decolorized with 1–4% sulfuric acid instead of the stronger acid-alcohol decolorant. The species of Nocardia are identified primarily by molecular methods such as 16S rRNA gene sequencing and restriction fragment length polymorphism (RFLP) analysis of amplified gene fragments such as hsp or secA.
Pathogenesis and Clinical Findings
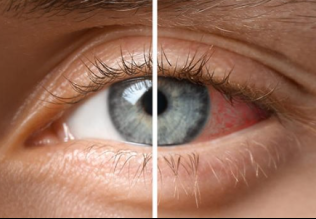
In most cases, nocardiosis is an opportunistic infection associated with several risk factors, most of which impair the cell-mediated immune responses, including corticosteroid treatment, immunosuppression, organ transplantation, AIDS, and alcoholism. Pulmonary nocardiosis is the main clinical presentation since inhalation is the primary route of bacterial exposure. A variety of symptoms may occur, including fever, night sweats, weight loss, chest pain, cough with or without sputum production, and shortness of breath. The clinical manifestations are not distinctive and mimic tuberculosis and other infections. Likewise, chest radiographs may show focal infiltrates, multifocal nodules, and even cavity formation. Pulmonary consolidations may develop, but granuloma formation and caseation are rare. The usual pathologic process is abscess formation (neutrophilic inflammation). Hematogenous spread from the lung often involves the central nervous system, where abscesses develop in the brain, leading to a variety of clinical presentations. Some patients have subclinical lung involvement and present with brain lesions. Dissemination may also occur to the skin, kidney, eye, or elsewhere.
Nocardia brasiliensis is associated with most primary cutaneous infections that usually result from trauma. These infections rarely disseminate.
Diagnostic Laboratory Tests
Specimens consist of sputum, pus, spinal fluid, and biopsy material. Gram-stained smears reveal gram-positive bacilli, coccobacillary cells, and branching filaments. With the modified acid-fast stain, most isolates will be acid fast. Nocardia species grow on most laboratory media. Serologic tests are not useful. Molecular methods are required for species-level identification, which is necessary for both epidemiologic and treatment purposes.
Treatment
The treatment of choice is trimethoprim–sulfamethoxazole. If patients fail to respond, a number of other antibiotics have been used with success, such as amikacin, imipenem, meropenem, fluoroquinolones, minocycline, linezolid, and cefotaxime. However, because the susceptibility patterns vary by species, susceptibility testing should be performed to guide treatment approaches. In addition to often prolonged antimicrobial treatment, surgical drainage or resection may be required.
Concept Checks
• Several members of the large group of aerobic Actinomycetes are modified acid-fast positive, most commonly Nocardia and R equi.
• Nocardia species are branching, beaded gram-positive rods found in soil and other environmental sources that cause systemic disease primarily in immunocompromised patients.
• Nocardia species are best identified after recovery on routine media by using molecular methods such as 16SrRNA gene or other gene target sequencing.
• Trimethoprim–sulfamethoxazole is the drug of choice for treatment of Nocardia infections. The use of other agents should be dictated by results of susceptibility testing.



|
|
|
|
السكر والملح وسرطان الجهاز الهضمي.. دراسة تحدد "صلة قوية"
|
|
|
|
|
|
|
روسيا تطلق صاروخا يحمل مركبة فضائية لأغراض دفاعية
|
|
|
|
|
|
|
في منطقة بين الحرمين الشريفين فرقة العباس (عليه السلام) تقيم مجلس ترحيم لمستشارها القانوي
|
|
|