آخر المواضيع المضافة

 النبات
الحيوان
الأحياء المجهرية
علم الأمراض
التقانة الإحيائية
التقنية الحيوية المكروبية
التقنية الحياتية النانوية
علم الأجنة
الأحياء الجزيئي
علم وظائف الأعضاء
الغدد
المضادات الحيوية
النبات
الحيوان
الأحياء المجهرية
علم الأمراض
التقانة الإحيائية
التقنية الحيوية المكروبية
التقنية الحياتية النانوية
علم الأجنة
الأحياء الجزيئي
علم وظائف الأعضاء
الغدد
المضادات الحيوية| Human Herpesvirus Types 6 And 7 |


|
|
Read More
Date: 10-11-2020
Date: 19-11-2015
Date: 20-11-2015
|
HHV-6 and HHV-7, classified as members of the Betaherpesvirinae, have marked similarities to HCMV in biologic and genome characteristics. Both HHV-6 and HHV-7 are causative agents of roseola infantum (exanthem subitum), although infection with HHV-7 is more frequently asymptomatic. Two variants of HHV-6 have been recognized: HHV-6A and HHV-6B. HHV-6B is virtually ubiquitous and is the causative agent of roseola infantum. HHV-6A has been implicated in the progression of HIV disease to full-blown AIDS.
A. Epidemiology and pathogenesis
Most infections with HHV-6 and HHV-7 occur during the first 3 years of life, with overall incidence of antibody approaching 90 per- cent of the population by age 3. Transmission is thought to be via oral secretions because the viruses replicate in the oropharynx as well as in B and T lymphocytes. HHV-7, in particular, is commonly recovered from healthy individuals' saliva. These viruses also infect peripheral blood lymphocytes and the cells of various solid organs. HHV-6A infection of lymphoid cells induces a number of significant cell responses, including the synthesis of CD4 glycoprotein, interferon-x, tumor necrosis factor-α, and interleukin-1-β. The ability of HHV-6A to induce expression of CD4 in cells not normally expressing it extends the range of cells that can be infected by HIV. In addition , HHV-6A transactivates transcription of HIV, accelerating the rate of cell death in coinfected cells. Latently infected cells are found among the peripheral blood lymphocyte population. HHV-6A was shown to accelerate AIDS progression in an animal model of the disease.
B. Clinical significance
HHV-6 infections resulting in disease are most common in infants and individuals who are immunocompromised.
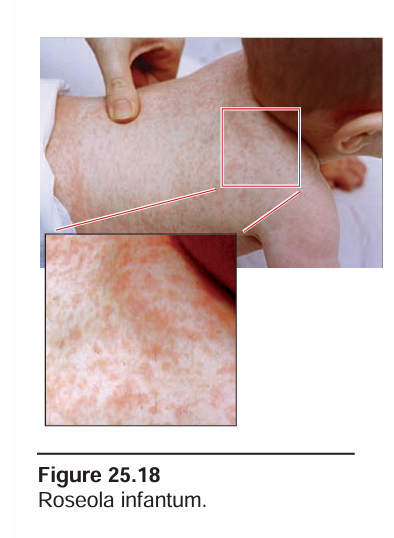
1. Primary infections: Symptomatic roseola infantum (exanthem subitum) occurs in roughly one third to one half of infants with a primary HHV-6 infection. It is characterized by a high fever of 3 to 5 days' duration, after which a characteristic erythematous macular rash appears on the neck and trunk, resolving after several more days without sequelae (Figure 25.18). HHV-7 infection has been shown to produce an identical clinical picture. Of greater clinical significance is that primary HHV-6 infection of infants is the cause of many acute febrile illnesses and febrile seizures in the absence of the characteristic rash. In some of these cases, HHV-7 has been shown to be the causative agent, whereas, in others, the patient was coinfected with both HHV-6 and HHV-7. Over 20 percent of emergency room visits for febrile illness in infants and one third of febrile seizures are caused by primary infection with HHV-6 and/or HHV-7 (Figure 25.19).

2. Recurrent infections: Following immunosuppression for organ transplantation or immunocompromise related to HIV infection, reactivation of latent HHV-6, frequently together with HCMV, has been associated with sometimes-fatal interstitial pneumonitis, fever, hepatitis, and encephalitis as well as with transplant rejection . The relationship of HHV-6A to AIDS has not been completely elucidated. Three factors may accelerate the progression from early HIV infection to terminal AIDS: 1) HHV-6A broadens the range of cell types infected by HIV by inducing CD4, 2) coinfected cells are killed more rapidly, and 3) extensively disseminated HHV-6A infection frequently occurs in terminal AIDS patients. The most common clinical syndrome associated with HHV-6 in AIDS patients is encephalitis (Figure 25.20).
C. Laboratory identification
A simple diagnostic test for primary infection with HHV-6 or HHV-7 is not available. PCR amplification has been used to demonstrate HHV-6 DNA in the CSF of patients with neurologic disease and in the serum of patients undergoing posttransplant reactivation of a latent infection.
D. Treatment and prevention
Because of its genetic relationship to HCMV, HHV-6 is generally inhibited by the same drugs (ganciclovir, cidofovir, and foscarnet), but extensive clinical trials have not yet been done. In AIDS patients, treatment of the HIV infection appears to reduce the amount of HHV-6 as well. No vaccine is currently available for these viruses.



|
|
|
|
4 أسباب تجعلك تضيف الزنجبيل إلى طعامك.. تعرف عليها
|
|
|
|
|
|
|
أكبر محطة للطاقة الكهرومائية في بريطانيا تستعد للانطلاق
|
|
|
|
|
|
|
العتبة العباسية المقدسة تبحث مع العتبة الحسينية المقدسة التنسيق المشترك لإقامة حفل تخرج طلبة الجامعات
|
|
|