آخر المواضيع المضافة

 النبات
الحيوان
الأحياء المجهرية
علم الأمراض
التقانة الإحيائية
التقنية الحيوية المكروبية
التقنية الحياتية النانوية
علم الأجنة
الأحياء الجزيئي
علم وظائف الأعضاء
الغدد
المضادات الحيوية
النبات
الحيوان
الأحياء المجهرية
علم الأمراض
التقانة الإحيائية
التقنية الحيوية المكروبية
التقنية الحياتية النانوية
علم الأجنة
الأحياء الجزيئي
علم وظائف الأعضاء
الغدد
المضادات الحيوية| Introduction to Antifungal Drugs |


|
|
Read More
Date: 31-3-2016
Date: 31-3-2016
Date: 31-3-2016
|
Introduction to Antifungal Drugs
Fungi rule their own kingdom. There are thou-sands of species of these saprophytic and parasitic organisms, but, as with bacteria, only a small minority are pathogens. Most pathogenic fungi are opportunistic and require a compromised host or disrupted barrier in order to cause infection in humans. In a way, the increase of systemic fungal infections can be seen as a medical advance, be-cause improvements in transplantation, oncology, rheumatology, neonatology, geriatrics, and other fields have created more hosts for fungi. The practice of medical mycology has expanded greatly.
Fungi exist in two basic forms: yeasts and moulds. Table 1 highlights some of the medically important fungi. Yeasts are solitary forms of fungi that reproduce by budding. When they are left to grow in colonies, they have a moist, shiny appearance. Moulds are multicellular fungi that consist of many branching hyphae and can reproduce either by translocation of existing hyphae to a new area, or through spore formation and spread (hence, one bad apple really does spoil a bunch). They have a familiar fuzzy appearance, such as the Rhizopus that you have undoubtedly seen on bread.
Table 1
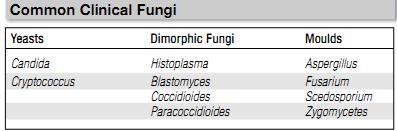
In addition to these two basic forms, there are dimorphic fungi that can exist in either form. These fungi are often mould-like at room temperature, but yeast-like at body temperature. They are also called endemic fungi, because they cause infections endemic to certain regions of the world; for example, Coccidioides immitis causes an infection in the southwestern United States and central California that is sometimes called valley fever.
Yeasts, particularly Candida species, have be-come the fourth leading cause of nosocomial blood-stream infections. This makes them important infectious agents that are worthy of our attention. Unfortunately, specific diagnostic criteria for invasive Candida infections are lacking. Moulds generally cause invasive disease only in immuno-compromised hosts, but they should be considered in patients with various levels of immune system suppression, not just those in the most severe category. Dimorphic fungi usually cause mild, self-limited disease, but some can also cause fatal disseminated disease, particularly in patients with suppressed immunity.
Antifungal pharmacotherapy has several problems that often make fungal infections more difficult to treat than bacterial infections. One is that fungal disease often presents no differently than bacterial disease, but the pathogens can be more difficult to isolate on culture. This makes the prompt initiation of empiric therapy important when invasive fungal infections are suspected. Prophylaxis is also used in highly susceptible populations to prevent fungal infections from developing.
Another concern with the treatment of fungal disease is that most centers do not conduct antifungal susceptibility testing. This forces clinicians to guess at likely susceptibility patterns based on speciation rather than test results. Further, the capabilities of the host significantly affect the likelihood of success in treating an invasive fungal infection. For neutropenic patients with mycoses, neutrophil recovery is a significant predictor of success, and patients with a prolonged immunocompromised status have a much worse prognosis. Therefore, while the selection of an appropriate antifungal is important, control of patient risk factors for fungal infection is perhaps more so, whether it is the need to remove a central venous catheter or to decrease doses of immunosuppressants.
Compared with the abundance of drugs avail-able to kill bacteria, the number of systemic anti-fungal drugs is much lower. Selective toxicity is more difficult to achieve with eukaryotic fungi than with prokaryotic bacteria. Several newly marketed agents have changed the way fungal infections are treated.
References
Gallagher ,J.C. and MacDougall ,c. (2012). Antibiotics Simplified. Second Edition. Jones & Bartlett Learning, LLC.



|
|
|
|
للعاملين في الليل.. حيلة صحية تجنبكم خطر هذا النوع من العمل
|
|
|
|
|
|
|
"ناسا" تحتفي برائد الفضاء السوفياتي يوري غاغارين
|
|
|
|
|
|
|
نحو شراكة وطنية متكاملة.. الأمين العام للعتبة الحسينية يبحث مع وكيل وزارة الخارجية آفاق التعاون المؤسسي
|
|
|