آخر المواضيع المضافة

 النبات
الحيوان
الأحياء المجهرية
علم الأمراض
التقانة الإحيائية
التقنية الحيوية المكروبية
التقنية الحياتية النانوية
علم الأجنة
الأحياء الجزيئي
علم وظائف الأعضاء
الغدد
المضادات الحيوية
النبات
الحيوان
الأحياء المجهرية
علم الأمراض
التقانة الإحيائية
التقنية الحيوية المكروبية
التقنية الحياتية النانوية
علم الأجنة
الأحياء الجزيئي
علم وظائف الأعضاء
الغدد
المضادات الحيوية| Pseudomonas aeruginosa |


|
|
Read More
Date: 2025-03-09
Date: 7-3-2016
Date: 7-3-2016
|
P. aeruginosa is widely distributed in nature and is commonly present in moist environments in hospitals. While not a part of the normal human microbiome, P. aeruginosa is capable of colonization of various body sites (eg, mucous membrane, respiratory tract, and GI tract). It is known to cause disease in humans, especially in people with altered and decreased host defenses (eg, neutropenia, chemotherapy, and burn wounds). The acquisition of the organism and subsequent infection can be either endogenous or exogenous. Endogenous infection occurs after colonization (eg, bacteremia after GI tract colonization); exogenous infection typically occurs from an environmental reservoir via a susceptible portal of entry (eg, burn wound infections or hot tub folliculitis).
Morphology and Identification
A. Typical Organisms
P. aeruginosa is motile and rod shaped, measuring about 0.6 × 2 µm (Figure 1). It is Gram-negative and occurs as single bacteria, in pairs, and occasionally in short chains.

Fig1. Gram-stain of P. aeruginosa, which are about 0.6 × 2 µm. Original magnification ×1000. (Courtesy of H Reyes.)
B. Culture
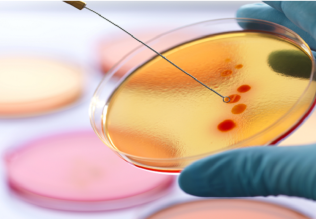
P. aeruginosa is an obligate aerobe that grows readily on many types of culture media, sometimes producing a sweet or grape-like or corn taco-like odor. Some strains hemolyze blood. P. aeruginosa forms smooth round colonies with a fluorescent greenish color. As mentioned above, many strains of P. aeruginosa produce a non-fluorescent bluish pigment, pyocyanin, which diffuses into the agar. As all fluorescent pseudomonads, P. aeruginosa also produces the fluorescent pigment pyoverdine, which gives a greenish color to the agar when combined with pyocyanin (Figure 2). Some strains may also produce a dark red pigment (pyorubin) or a brown black pigment (pyomelanin).

Fig2. P. aeruginosa on a 10-cm Mueller-Hinton agar plate. Individual colonies are 3–4 mm in diameter. The organism produces pyocyanin, which is blue, and pyoverdine, which is green. Together these pigments produce the blue-green color that is seen in the agar around the pseudomonas growth. (Courtesy of S Lowe.)
P. aeruginosa in culture can produce multiple colony types (Figure 3); isolates from different colony types may also have different biochemical and enzymatic activities and different antimicrobial susceptibility patterns. Sometimes, it may not be clear if the colony types represent different strains of P. aeruginosa or are variants of the same strain. Cultures from patients with cystic fibrosis (CF) often yield P. aeruginosa organisms that form mucoid colonies as a result of overproduction of alginate, an exopolysaccharide. In CF patients, the exopolysaccharide appears to provide the matrix for the organisms to live in a biofilm .

Fig3. Variation in colony morphology of P. aeruginosa. A: Green-gray colonies 6–8 mm in diameter on a 10-cm blood agar plate; the blood in the agar around the colonies shows hemolysis. B: Silver-toned dry colonies on a similar blood agar plate; no hemolysis is present (the dark shadow in the lower part of the picture is from a label on the back of the Petri dish). (Courtesy of H Reyes.)
C. Growth Characteristics
P. aeruginosa grows well at 37°C to 42°C; its growth at 42°C helps differentiate it from other Pseudomonas species that produce fluorescent pigments. P. aeruginosa, like all pseudomonads, does not ferment carbohydrates, but many strains oxidize glucose; these organisms are therefore oxidase positive. Identification is usually based on colonial morphology, the presence of characteristic pigments, oxidase positivity, and growth at 42°C. Differentiation of P. aeruginosa from other pseudomonads on the basis of biochemical activity requires testing with a large battery of substrates.
Antigenic Structure and Toxins
Pseudomonads, and P. aeruginosa specifically, produce a variety of virulence factors, including adhesins, enzymes, and toxins. Pili (fimbriae) extend from the cell surface and promote attachment to host epithelial cells. An exopolysaccharide, alginate, is responsible for the mucoid colonies seen in cultures from patients with CF. Lipopolysaccharide, which exists in multiple immunotypes, is responsible for many of the endotoxic properties of the organism. P. aeruginosa can be typed by lipopolysaccharide immunotype and by pyocin (bacteriocin) susceptibility. Most P. aeruginosa isolates from clinical infections produce extracellular enzymes, including elastases, pro teases, and two hemolysins (a heat-labile phospholipase C and a heat-stable glycolipid). In addition, pyocyanin produced by P. aeruginosa is responsible for the production of hydrogen peroxide and superoxide, and stimulates the release of interleukin (IL)-8. The increased release of IL-8 serves as an attractant for neutrophils. The other pigment, pyoverdine, serves as a siderophore, that is, binds iron.
Many strains of P. aeruginosa produce exotoxin A, which causes tissue necrosis and is lethal for animals when injected in purified form. The toxin blocks protein synthesis by a mechanism of action identical to that of diphtheria toxin, although the structures of the two toxins are not identical. Antitoxins to exotoxin A are found in some human sera, including those of patients who have recovered from serious P. aeruginosa infections.
P. aeruginosa produces four type III-secreted toxins that cause cell death or interfere with the host immune response to infection. Exoenzyme S and exoenzyme T are bifunctional enzymes with GTPase and ADP-ribosyl transferase activity, exoenzyme U is a phospholipase, and exoenzyme Y is an adenylyl cyclase.
Pathogenesis
P. aeruginosa is pathogenic only when introduced into areas devoid of normal defenses, such as when mucous mem branes and skin are disrupted by direct tissue damage as in the case of burn wounds; when intravenous or urinary catheters are used; or when neutropenia is present, as in cancer chemotherapy. The bacterium attaches to and colonizes the mucous membranes or skin, invades locally, and subsequently produces systemic disease (eg, bloodstream infections). These processes are promoted by the pili, enzymes, and toxins described earlier. Lipopolysaccharide plays a direct role in causing fever, shock, oliguria, leukocytosis and leukopenia, disseminated intravascular coagulation, and adult respiratory distress syndrome. The propensity to form biofilms by P. aeruginosa in the lumen of catheters and in the lungs of CF patients greatly contributes to the virulence of this organism.
P. aeruginosa and other pseudomonads are resistant to many antimicrobial agents and therefore may become dominant and overgrow the more susceptible bacteria that are part of the normal microbiota and are suppressed.
Clinical Findings
P. aeruginosa produces infection of wounds and burns, often giving rise to blue-green pus; meningitis when introduced by lumbar puncture or during a neurosurgical procedure; and urinary tract infection when introduced by catheters and instruments or in irrigating solutions. Involvement of the respiratory tract, especially from contaminated respirators, results in necrotizing pneumonia. In CF patients, P. aeruginosa causes a chronic pneumonia, a significant cause of morbidity and mortality in this population. The bacterium is often found in mild otitis externa in swimmers. It may cause invasive (malignant) otitis externa in patients with diabetes. Infection of the eye, which may lead to rapid destruction of the eye, occurs most commonly after injury or surgical procedures. In infants or debilitated persons, P. aeruginosa may invade the bloodstream and result in fatal sepsis; this occurs commonly in patients with leukemia or lymphoma who have received antineoplastic drugs or radiation therapy and in patients with severe burns. In most P. aeruginosa infections, the symptoms and signs are nonspecific and are related to the organ involved. Occasionally, verdoglobin (a breakdown product of hemoglobin) or fluorescent pigment can be detected in wounds, burns, or urine by ultraviolet fluorescence. Hemorrhagic necrosis of skin occurs often in sepsis caused by P. aeruginosa; the lesions, called ecthyma gangrenosum, are surrounded by erythema and often do not contain pus. P. aeruginosa can be seen on Gram-stained specimens from ecthyma lesions, and culture results are positive. Ecthyma gangrenosum is uncommon in bacteremia caused by organisms other than P. aeruginosa. A form of folliculitis associated with poorly chlorinated hot tubs and swimming pools can be seen in otherwise healthy persons.
Diagnostic Laboratory Tests
A. Specimens
Specimens from skin lesions, pus, urine, blood, spinal fluid, sputum, and other material should be obtained as indicated by the type of infection.
B. Smears Gram-negative rods are often seen in smears. No specific morphologic characteristics differentiate pseudomonads in specimens from enteric or other Gram-negative rods.
C. Culture Specimens are plated on blood agar and the differential media commonly used to grow the enteric Gram-negative rods. Pseudomonads grow readily on most of these media, but they may grow more slowly than the enterics. P. aeruginosa does not ferment carbohydrates, including lactose, and is easily differentiated from the lactose-fermenting bacteria. Culture is the specific test for diagnosis of P. aeruginosa infection. P. aeruginosa can be presumptively identified as described above; however, definitive identification, as well as differentiation from and identification of other pseudomonads, requires a battery of biochemical tests. Various manual as well as automated commercial test systems are available. In recent years, MALDI-TOF MS has been shown to reliably identify the various fluorescent and non-fluorescent pseudomonads.
Treatment
Traditionally, treatment of P. aeruginosa infections with a single antibiotic has not been recommended; a combination antimicrobial therapy is usually required to successfully treat significant infections. There are two reasons why antimicrobial therapy of serious P. aeruginosa infections can be challenging: patients with P. aeruginosa infections are typically immunocompromised, and in addition, the organism itself is frequently resistant to multiple different classes of antimicrobial agents. An extended-spectrum penicillin, such as piperacillin active against P. aeruginosa, is typically used in combination with an aminoglycoside, usually tobramycin. Other drugs active against P. aeruginosa include aztreonam; carbapenems such as imipenem or meropenem; and the fluoroquinolones, including ciprofloxacin. Of the cephalosporins, ceftazidime, cefoperazone, and cefepime are active against P. aeruginosa; ceftazidime is often used with an aminoglycoside in primary therapy of P. aeruginosa infections, especially in patients with neutropenia.
P. aeruginosa is intrinsically resistant to many antimicrobial agents, and can acquire additional resistance to many other antimicrobial agents via horizontal gene transfer and/or mutations. The mechanisms responsible for intrinsic resistance include various multidrug efflux pumps (eg, affecting β-lactams, fluoroquinolones, macrolides, and other antibiotics), as well as an inducible chromosomal AmpC β-lactamase (resistance to ampicillin, amoxicillin, amoxicillin-clavulanate, first- and second-generation cephalosporins, as well as ceftriaxone and cefotaxime). The susceptibility/ resistance patterns of P. aeruginosa vary geographically, and antimicrobial susceptibility testing (AST) should be routinely performed to support the choice of antimicrobial therapy and hospital antibiotic stewardship programs. In addition, multi drug resistance has become a major issue in the management of hospital-acquired infections with P. aeruginosa because of acquisition of chromosomal β-lactamases, extended spectrum β-lactamases, carbapenemases, porin channel mutations, and efflux pumps. The percentage of P. aeruginosa isolates that are multidrug resistant varies considerably (50%) by region and country.
Epidemiology and Control
P. aeruginosa is primarily a nosocomial, opportunistic pathogen, and the methods for control of infection are similar to those for other nosocomial pathogens. According to data from the National Healthcare Safety Network (NHSN), P. aeruginosa is currently the fifth most common pathogen implicated in hospital-acquired infections in the United States. Infection rates are especially high in the ICU setting and in long-term acute care hospitals. Because Pseudomonas species thrive in moist environments, special attention should be paid to sinks, water baths, showers, hot tubs, and other wet areas. However, given the organism’s ubiquitous presence in the hospital environment, all attempts to eliminate its presence are practically ineffective. Instead, effective infection-control prevention measures should focus on preventing the contamination of medical equipment, potential cross-contamination between patients, and selection of appropriate antibiotic therapy guidelines to prevent emergence of drug resistance. For epidemiologic purposes, strains of P. aeruginosa can be typed using molecular typing techniques; these techniques are especially useful during “outbreak” investigations.



|
|
|
|
"إنقاص الوزن".. مشروب تقليدي قد يتفوق على حقن "أوزيمبيك"
|
|
|
|
|
|
|
الصين تحقق اختراقا بطائرة مسيرة مزودة بالذكاء الاصطناعي
|
|
|
|
|
|
|
مكتب السيد السيستاني يعزي أهالي الأحساء بوفاة العلامة الشيخ جواد الدندن
|
|
|